

The data supporting the use of opioids to treat chronic, non-cancer pain is quite weak, says Michael Ashburn, director of the Penn Pain Medicine Center at the Perelman School of Medicine. As few as one in five patients may have clinically meaningful pain relief six months after being placed on opioids, and the average pain relief that people experience if they do respond is 30-40%.
“Unfortunately, both physicians and patients have a misperception that opioids are very effective for the treatment of pain—particularly chronic pain—and if dosed properly, patients will get complete or near complete pain relief,” says Ashburn, who is also a professor of anesthesiology and critical care at the Hospital of the University of Pennsylvania (HUP). “And both perceptions are completely wrong. Opioids only work in a small percentage of patients who have chronic pain, and when they work, they rarely are associated with significant pain relief, but only modest or moderate pain relief.”
Nevertheless, here we are, in the midst of an opioid epidemic in the United States that has claimed nearly 400,000 lives so far in the 21st century. Ninety percent of individuals who have an opioid use disorder are misusing prescription drugs.
Ashburn says there is no simple answer for how we got here. He says the rapid uptake in opioid use that began in the 1990s and early 2000s resulted from a confluence of events, including aggressive marketing by the pharmaceutical industry, the fragmentation of the health care system, health care providers grossly underestimating the risk of harm from opioids, the lack of funding for pain-related clinical research, and well-intended but improper advocacy by proponents of improved pain control.
“There’s a lot of blame to go around,” he says.
The challenge of integrated pain care
Among pain specialists, Ashburn says there is an assertion that medical professionals defaulted to opioids when the payment structure for modern medical care made it increasingly difficult to offer proper, integrated pain care.
If a doctor was unable to get a patient to see a physical therapist, pain psychologist, pain specialist, and occupational therapist, and get prior authorization or access to effective pain care, he or she took the less-challenging but well-meaning route and ended up overprescribing opioids.
Martin Cheatle, director of behavioral medicine at the Pain Medicine Center and an associate professor of psychology in psychiatry at HUP, says pain care in the United States has “devolved, not evolved.”
In the past, patients would have access to an interdisciplinary pain program that would offer a multimodal approach to improving their pain and quality of life, which would include physical therapy, occupational therapy, medical care, behavioral health, nutrition, and medication trials.
“There was a team approach, with a shared treatment philosophy and clinical decision-making,” Cheatle says.
In the late 1990s, there were approximately a thousand of these interdisciplinary pain facilities across the country—but he says there are only about 20 to 30 still in operation due to health care reimbursement issues.
“In the current environment, we have to patch together a multidisciplinary approach for each patient we care for at the Pain Medicine Center,” says Cheatle, who is also director of pain and chemical dependency research at Penn Medicine’s Center for Studies of Addiction. “Dr. Ashburn and Dr. Lee Fleisher [chair of the Department of Anesthesiology and Critical Care] have been working diligently to promote and reinstitute a multidisciplinary approach to pain care. But it is a daunting mission due to reimbursement barriers.”
The good news is that there has been slow, steady progress toward addressing some of these issues. For instance, the Pain Medicine Center is actively discussing with specific health insurance companies the idea of having a novel payment rate to allow them to provide integrated care.
In addition, the Center has been working for years on developing a closer relationship with their physical therapy and occupational therapy partners, and exploring innovative ways of providing physical therapy services to patients as close to home as possible. Since 2007, the Center has expanded from one location to eight, serving patients from Cherry Hill to Chester County Hospital.
Opioids in the community
Around the time of surgery, the risk of harm associated with prescribing opioids is multifactorial. There is risk to the person receiving the drugs if given improperly, but also a risk of harm to his or her family and the community, if the drugs are not stored or disposed of correctly.
Ashburn says there is data that shows that the number of opioids that are prescribed in a community is correlated with the death rate of overdose opioid deaths.
“I believe that there’s a link between how doctors prescribe these medications and the community death rate from overdoses,” he says.
A team of researchers and clinicians at Penn, including Ashburn, has been carefully looking at common, high-volume surgical procedures to determine best practices on how to manage pain using a multitude of different treatments, such as regional aesthetic techniques, acetaminophen (Tylenol), anti-inflammatory medications, and very judicious use of low doses of opioids for a short period of time to avoid excessive prescribing of opioids.
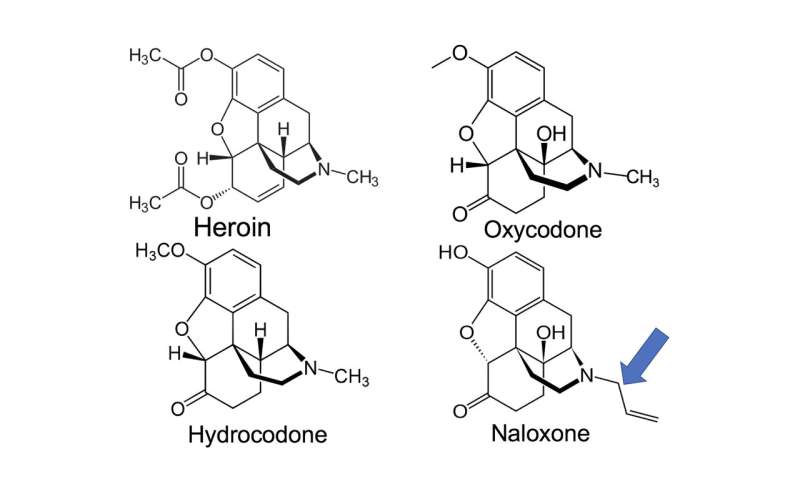
“Most people don’t understand that when we think of the face of opioid addiction, we think of the individual in Kensington who’s injecting,” says Ashburn. “But only 10% of the people who have an opioid use disorder use heroin. The vast majority of people who have an opioid use disorder are using prescription drugs for nonmedical purposes, so the risk that a provider has to worry about is the risk to the patient in front of them, the risk to that patient’s family, and the risk to their local community.”
Pennsylvania has guidelines on how opioids should be used for chronic, non-cancer pain, and recently published a new guideline on how opioids should be used in dental practice, a document Ashburn helped revise.
“In general, opioids are not proper to prescribe after most dental procedures,” he says.
Opioid use in dental medicine
The majority of 17- to 21-year-olds in the United States are first exposed to opioids when they receive pain medication after getting their wisdom teeth removed—some 5 million cases per year. The teeth must be surgically extracted, a procedure that involves soft tissue and bone trauma.
Elliot V. Hersh, a professor in the Department of Oral and Maxillofacial Surgery/Pharmacology at the School of Dental Medicine, says the process of removing wisdom teeth closely resembles an orthopedic surgery procedure, and is probably the most traumatic of all outpatient dental surgical procedures.
In 2011, dentists, including oral surgeons, were the No. 2 prescribers of immediate release opioids in the United States among health care specialties, most frequently prescribing Vicodin (acetaminophen plus hydrocodone), Percocet (acetaminophen plus oxycodone) and Tylenol No. 3 (acetaminophen plus codeine).
Non-opioids, though, are more effective than opioids in treating post-surgical dental pain.
Hersh says post-surgical dental pain is mainly driven by inflammation, and non-steroidal anti-inflammatory drugs (NSAIDs), as their name suggests, target inflammation and reduce pain more effectively than pure opioids.
“In post-surgical dental pain, they work at least as well, if not better, than two Tylenol No. 3s, and work better than a single Percocet,” he says.
Studies showing that NSAIDs are more effective than opioids in treating post-surgical dental pain have been around since the 1980s and ’90s, but until recently, Hersh says oral surgeons and some other dentists almost reflexively prescribed opioids combined with acetaminophen as their primary pain relievers.
This conundrum persisted for several reasons, one of which is the fact that dental specialists who were trained in the 1970s and ’80s were taught to prescribe acetaminophen-plus-opioid combinations to relieve pain and did not read the updated literature and/or decide to change their prescribing practices.
Furthermore, oral surgeons and dentists are writing prescriptions for pain when patients are still numb—a practice somewhat unique to the field of dentistry. Hersh says they often prescribe for the worst-case scenario, basing their prescriptions on how long the procedure took and how invasive the procedure was, without certainty about how much post-operative pain a patient is going to experience once the local anesthesia wears off.
(At Penn Dental Medicine, students have been taught since the late 1980s that NSAIDs are the drugs of choice for post-surgical dental pain.)
Patient expectations are also a factor. Hersh says some patients falsely believe that NSAIDs like ibuprofen and naproxen sodium are not as strong and effective as opioids because they are available over-the-counter at lower doses.
Dentists are no longer the No. 2 prescribers of immediately release opioids; since their zenith in 2011, they have fallen to sixth. Progress, Hersh says, but still too high.
He says the environment changed due to articles and commentaries written by himself and his colleagues, mandatory continuing education requirements on the topic for biannual relicensure, and also because of the establishment of the Prescription Drug Monitoring Program.
The oral surgeons of today will typically recommend or prescribe an NSAID for post-surgical pain—but may still, in the most traumatic cases, prescribe an opioid as well. If they do, Hersh says patients should be prescribed a small number for limited duration.
“And what I mean by limited duration is probably no more than two days’ worth,” he says.
Opioids and veterinary medicine
Inpatients at Ryan Hospital at the School of Veterinary Medicine are often given injectable opioid medications like fentanyl, hydromorphone, methadone, and buprenorphine to relieve pain.
Dana Clarke, an assistant professor of interventional radiology at Penn Vet, says opioids are essential for managing pain in animals in the hospital. Dogs can be given NSAIDs, but are more sensitive to the drugs than humans, especially dogs with liver or kidney disease. Birds and rabbits can be given NSAIDs, too. They are generally avoided in cats however, due to their hypersensitive kidneys and livers.
“In people, [doctors] can rely on NSAIDs so much more heavily,” Clarke says. “We just don’t have that ability to rely on them as heavily due to species differences and sensitivities.”
Human medicine contains comprehensive documentation on the number and type of controlled drugs, such as opioids, that doctors are prescribing. Clarke says veterinarians track controlled drugs as well, logging all drugs used with the Drug Enforcement Administration and maintaining accurate records of the amounts and frequency of medications being dispensed for every patient. Vets do not, on the other hand, have a national database/registry as they do in human medicine to know what is being prescribed to a given pet from state to state.
To get a sense of the controlled drug prescribing practices of veterinarians at Penn Vet, and set a baseline for future reference, Clarke, Kenneth J. Drobatz, a professor of critical care at Penn Vet, and research volunteer Chloe Korzekwa conducted a cross-sectional study that inventoried all opioid tablets and/or patches dispensed or prescribed by doctors at Ryan Hospital for small animals and species from Jan. 1, 2007, to Dec. 21, 2017. The study included 134 veterinarians with 366,468 visits.
Published in JAMA Network Open, the researchers found that, over a 10-year period, veterinarians at Ryan Hospital prescribed 1,051,836 tablets of tramadol, 97,547 tablets of hydrocodone, 38,939 tablets of codeine, and 3,153 fentanyl patches to dogs (73.0%), cats (22.5%), and exotic animals (4.5%).
The study, Clarke says, raised some interesting questions about the large number of opioids prescribed, but was designed to be more informative about the overall number than to draw any big conclusions.
She says it is important to note that Ryan Hospital—a large teaching and specialty hospital— handles much more advanced cases than the average veterinary practice, including animals with major trauma and patients that have a chronic condition that requires opioids.
“A lot of the dogs that I treat with tracheal collapse have to be on hydrocodone for their lifetime to prevent the cough,” she says.
Concerns about what could happen once drugs left the building was one of the reasons the researchers embarked on the study, Clarke says. They do not have proof that some owners may be abusing their pets’ opioids, but she says the opioids prescribed to animals are the same ones used in humans, albeit in different doses.
Even before the study was published, Clarke says Penn Vet has been trying to minimize the use of injectable pain medication in favor of non-opioid medications and local anesthetics, if possible, in small animals, particularly given concerns about the impacts of these medications on their gastrointestinal tract. They are also thoughtful about the amount of opioids sent home with pets after surgery or other procedures.
“Don’t send 10 days when they only need three days, and we are trying to be really, really smart about how much we’re sending, where it’s going, and trying to limit any chances for diversion to somewhere else,” she says, “because unfortunately you have to think about those things as the reality of the current opioid crisis.”
The future of pain control
In this age of the opioid epidemic, Ashburn says it is important not to be “opiophobic.” He says the management of patients on opioids is something they do every day at the Pain Medicine Center—but they so in “a very, thoughtful, careful, diligent way that lowers the risk of harm to the patients that we prescribe these medications to.”
Health professionals within the Penn community have developed integrated pathways to provide multimodal care, including many different non-opioid medications, regional anesthetics, and changes in the conduct of the anesthesia, which have led to much less reliance on opioids after surgery.
Nabil Elkassabany, an associate professor of anesthesiology and critical care at HUP, has developed an integrated anesthesia and pain treatment plan for individuals undergoing major shoulder surgery that requires little to no use of opioids after surgery.
Ashburn says similar efforts are being developed implemented for providing better pain control in individuals undergoing foot and ankle surgery, knee surgery, orthopedic trauma surgery, and a caesarean section.
Source: Read Full Article