. DOI: 10.2196/36477")
Stroke is among the most dangerous and commonly misdiagnosed medical conditions. Black and Hispanic people, women, older people on Medicare, and people in rural areas are less likely to be diagnosed in time for treatment to be effective. In a new study, researchers used machine learning methods and data available when patients enter the hospital to develop a model that predicts strokes with more accuracy than current models.
The study, by researchers at Carnegie Mellon University (CMU), Florida International University (FIU), and Santa Clara University (SCU), appears in the Journal of Medical Internet Research.
Diagnostic errors are a significant public health problem, and preventable deaths from stroke due to such errors occur more than 30 times more often than deaths from myocardial infarction. Diagnosing stroke is difficult due to the numerous conditions that mimic stroke, such as seizures, migraines, and alcohol intoxication. These difficulties can lead to delays, which can compound health issues.
An automated screening tool to analyze available data and suggest a stroke diagnosis has significant potential to help address this problem. Scientists have turned to artificial intelligence and machine learning to identify hidden insights from a large volume of data and generate predictions for new patients.
“Machine learning methods have been used to help detect stroke by interpreting detailed data such as clinical notes and diagnostic imaging results,” explains Rema Padman, Trustees professor of management science and healthcare informatics at CMU’s Heinz College, who coauthored the study. “But such information may not be readily available when patients are initially triaged in hospital emergency departments, especially in rural and underserved communities.”
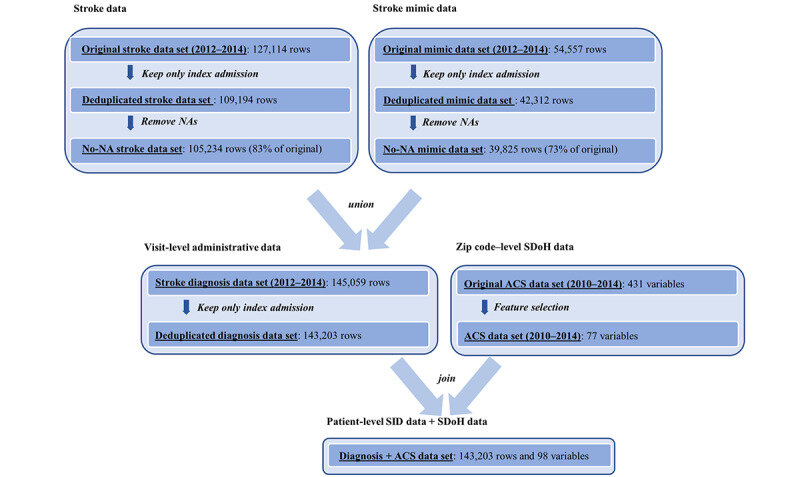
Padman and her colleagues sought to develop a stroke prediction algorithm based on data that are widely available upon patient admission. They also assessed the added value of social determinants of health (SDoH) in predicting strokes; these include the conditions people are born into, grow up in, live in, and age in, and the drivers of these conditions.
Their study examined more than 143,000 hospital visits of unique patients seen in Florida acute care hospitals from 2012 to 2014. The researchers also looked at SDoH data from the U.S. Census’s American Community Survey. Their model incorporated variables that are routinely collected by health care providers and payers upon entry to a hospital, such as basic demographics (age, gender, race, ethnicity), number of chronic conditions, and primary payer (e.g., Medicare, Medicaid or private insurance).
The researchers’ model was accurate (84% precision in predicting strokes) and sensitive, outperforming existing scales (which tend to miss up to 30% of strokes). Use of the model suggests it is possible to predict the likelihood of a patient’s condition being stroke at the time of hospital presentation based on patients’ demographics and social determinants of health that are available at the time of entry into the hospital, before obtaining diagnostic imaging or laboratory test results, say the authors.
“Existing models’ moderate sensitivity raises concerns that they miss a substantial percentage of people with stroke,” explains Min Chen, associate professor of information systems and business analytics in FIU’s College of Business, who co-authored the study.
“In hospitals with a shortage of medical resources and clinical staff, our algorithm can supplement current models to help quickly prioritize patients for appropriate intervention.”
“Because our model doesn’t require clinical notes or diagnostic test results, it might be particularly useful in addressing the misdiagnosis challenges when dealing with walk-in patients with stroke with milder and atypical symptoms,” suggests Xuan Tan, lecturer in information systems and analytics in the Leavey School of Business at SCU, another co-author of the study.
“It could also be useful in low-volume or non-stroke centers’ emergency departments, where providers have limited daily exposure to stroke, and in rural areas with limited availability of sensitive diagnostic tools.”
Among the study’s limitations, the authors note that since their study was retrospective, confirming stroke cases relied on International Classification of Diseases codes and did not involve reviewing patients’ records. In addition, they caution that their algorithm should not be considered as a gold standard for stroke diagnosis, but rather as a model that complements existing stroke scoring systems used in hospitals. Finally, their findings are limited by social determinants of health variables available in administrative data.
More information:
Min Chen et al, A Machine Learning Approach to Support Urgent Stroke Triage Using Administrative Data and Social Determinants of Health at Hospital Presentation: Retrospective Study, Journal of Medical Internet Research (2023). DOI: 10.2196/36477
Journal information:
Journal of Medical Internet Research
Source: Read Full Article